
National Standards of Healthcare Cleanliness 2021 Explained for GP Practices
This guide has been reviewed and updated in 2026 to reflect current NHS expectations, audit requirements and infection prevention alignment within primary care settings.
Since full compliance became mandatory in November 2022, the National Standards of Healthcare Cleanliness 2021 have formed the benchmark for cleanliness across NHS healthcare environments.
For GP surgeries and primary care settings, these standards are more than operational guidance. They underpin infection prevention frameworks, support regulatory compliance and may be reviewed during inspections by Care Quality Commission.
As a contractor delivering structured GP Surgery Cleaning across Essex and Suffolk, we are frequently asked how these NHS cleaning standards apply in real-world primary care environments. This guide explains the framework clearly and practically.
What Are the National Standards of Healthcare Cleanliness 2021?
The National Standards of Healthcare Cleanliness 2021 replaced the 2007 National Specifications for Cleanliness. Introduced by NHS England, the updated framework created a more measurable, risk-based and transparent approach to healthcare cleaning.
The standards introduced:
- Functional Risk categories (FR1–FR6)
- A Commitment to Cleanliness Charter
- Structured technical and efficacy audits
- Star ratings (where applicable)
- Outcome-based cleaning frequencies
- Clear documentation requirements
Unlike previous guidance, the 2021 standards emphasise evidence, accountability and measurable performance, not just routine cleaning tasks.
Functional Risk Categories (A–F) in GP Surgeries & How To Apply Them in Practice
One of the most significant updates introduced under the National Standards of Healthcare Cleanliness 2021 was the requirement to classify all areas within a healthcare environment using Functional Risk Categories (FRCs). Rather than treating every space the same, the standards require each room to be assessed according to infection risk.
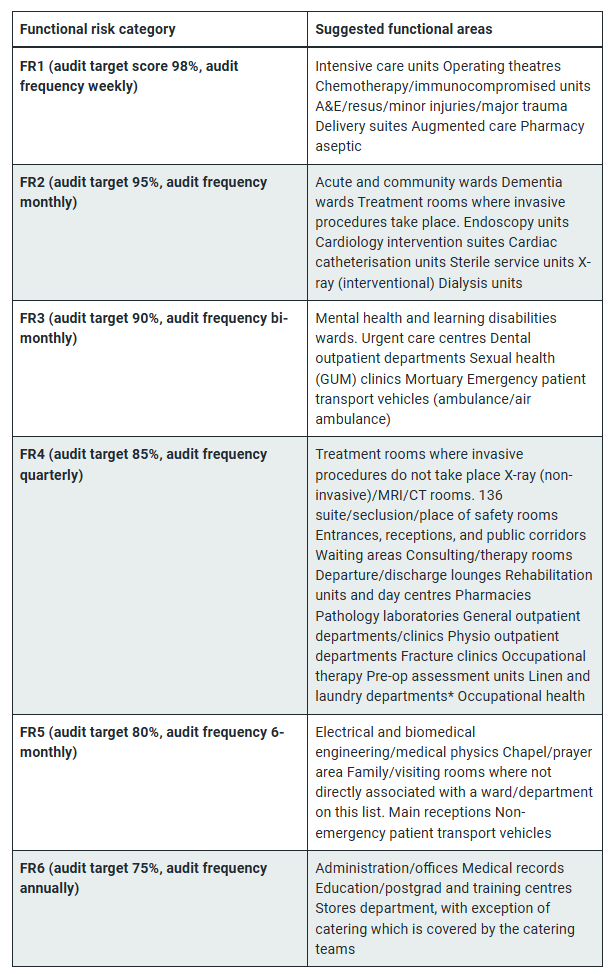
The six categories range from:
- FR1 – Very high risk — Areas with the greatest infection risk requiring the most frequent cleaning and auditing (e.g., major surgical or invasive procedure spaces).
- FR2 – High risk — Areas with significant patient contact and clinical activity (e.g., some treatment rooms).
- FR3 – Medium risk — Clinical support areas or rooms with moderate exposure.
- FR4 – Lower–medium risk — Areas with less patient contact but still clinical relevance.
- FR5 – Low risk — Non-clinical areas, often with minimal patient exposure.
- FR6 – Very low risk — Administrative zones or back-office areas
In a typical GP surgery, Functional Risk categorisation may look like:
- Treatment rooms – FR2
- Minor procedure rooms – FR2
- Consulting rooms – FR3 or FR4
- Waiting areas and reception – FR5
- Offices and back-of-house areas – FR6
Each category carries defined cleaning frequencies and performance expectations under NHS guidance. Understanding the categories is one thing. Embedding them operationally is another. At Peak Commercial Cleaning, we incorporate Functional Risk Categories directly into our daily cleaning systems.
This includes:
- Assigning an FRC classification to every room during our site assessment
- Building tailored, surgery-specific cleaning checklists aligned to each category
- Adjusting cleaning frequencies according to risk level
- Ensuring higher-risk areas receive enhanced attention and oversight
- Reflecting FRC allocation within audit documentation
Rather than using a generic commercial cleaning template, each GP surgery receives a bespoke specification aligned to its clinical layout and infection prevention requirements. During our initial site visit, we review:
- Room usage
- Clinical activity levels
- Patient flow
- Waste management processes
- Existing IPC policies
From there, we produce a structured cleaning plan built around Functional Risk Categories and compliant frequencies. This approach ensures that the standards are not just understood, they are actively embedded into daily cleaning checklists, supervision processes and audit systems.
If you are reviewing your current GP surgery cleaning arrangements, we would recommend beginning with a structured site visit to assess room categorisation and ensure alignment with the NHS standards. Click here to book a site visit.
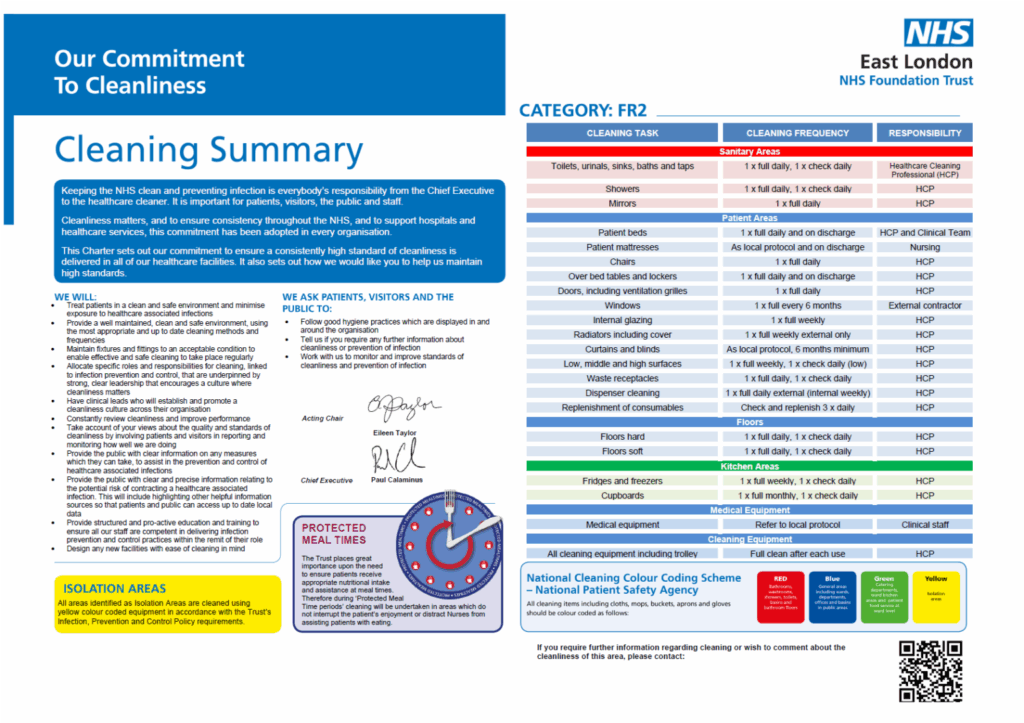
Commitment to Cleanliness Charter
Under the standards, healthcare providers are expected to publicly display a Commitment to Cleanliness Charter in a patient-facing area.
The charter confirms the organisation’s commitment to maintaining safe and hygienic environments. It promotes transparency and reinforces accountability to patients, staff and visitors.
For GP practices, this visible pledge strengthens patient confidence and demonstrates alignment with NHS cleanliness standards.
The GP Surgery Cleaning Audit Process
The National Standards of Healthcare Cleanliness require a structured audit framework to ensure cleaning standards are measurable and evidenced. Under the framework, three types of audits apply: Technical, Efficacy and External. At Peak Commercial Cleaning, we have embedded these audit requirements directly into our healthcare cleaning model.
The 50-point technical audit assesses whether areas meet the defined cleanliness standard linked to their assigned Functional Risk (FR1-FR6) category. In practice, this means:
- Each room is audited against the correct performance standard for its FR category.
- Higher-risk areas (e.g. FR2 treatment rooms) are audited more rigorously.
- Results are recorded and scored.
- Any failures trigger corrective actions.
When it comes to technical audits, every healthcare site we manage is assigned a dedicated Area Manager who oversees scheduled audits in line with the Functional Risk (FR1-FR6) profile of the surgery. Audit frequency and scrutiny levels are aligned to the infection risk associated with each area, ensuring higher-risk clinical rooms receive proportionate oversight. Findings from each audit are formally documented, with any required remedial actions logged and followed through to completion. Where recurring trends are identified, these are escalated and reviewed at management level to ensure continuous improvement. This structured approach ensures that cleanliness is not assumed – it is measured, recorded and verified.
While technical audits assess the outcome of cleaning, efficacy audits focus on how cleaning is delivered. These reviews evaluate adherence to correct PPE usage, compliance with colour coding systems, proper COSHH management and chemical storage, staff training and competency records, uniform standards, and complaint response procedures. At Peak Cleaning we conduct structured regular reviews of cleaning processes to ensure they remain aligned with healthcare best practice and infection prevention expectations.
During these reviews, training documentation is assessed, chemical storage arrangements are inspected, and compliance with established cleaning protocols is verified. All findings are documented and retained for governance purposes, providing clear evidence of process control. This ensures that our teams are not only achieving the required cleaning standards but are consistently following correct healthcare cleaning procedures in line with NHS expectations.
External audits provide independent validation where applicable under local governance arrangements. While these are typically arranged by the healthcare provider, we actively support the process by:
- Providing requested documentation
- Sharing audit records
- Responding to feedback
- Implementing improvement actions where required
How NHS Cleaning Standards Link to CQC Compliance
While the CQC does not directly enforce the National Standards of Healthcare Cleanliness, inspectors may review evidence of:
- Risk categorisation
- Cleaning specifications
- Audit records
- Infection prevention alignment
- Staff training documentation
Failure to demonstrate a structured, risk-based cleaning framework can raise compliance concerns under safety and infection control regulations. For GP surgeries, working with a contractor who understands NHS standards supports inspection readiness.
At Peak Commercial Cleaning, we have a proven track record of inspection readiness. Contact us to arrange a free quote.
Why a Detailed Cleaning Specification Is Essential
A compliant healthcare cleaning specification should clearly outline:
- Functional Risk Category allocation
- Cleaning frequencies
- Defined tasks
- Responsible personnel
- Waste handling processes
- Audit arrangements
- Escalation procedures
This document must align with the practice’s Infection Prevention & Control (IPC) policy. A generic office cleaning schedule is not sufficient in a healthcare environment. Our approach to surrounding areas is built around structured specifications designed specifically for primary care environments.
What GP Practices Should Look for in a Cleaning Contractor
When reviewing healthcare cleaning arrangements, practices should consider:
- Does the contractor understand Functional Risk Categories?
- Can they evidence technical and efficacy audits?
- Are staff trained specifically in healthcare cleaning?
- Is COSHH compliance documented?
- Can they support you during CQC inspections?
Healthcare cleaning is not standard commercial cleaning. It requires structured systems, oversight and documented processes.
Summary
The National Standards of Healthcare Cleanliness 2021 introduced a measurable, risk-based framework for healthcare environments. While the structure has not been replaced since 2022, expectations around documentation, audit evidence and infection prevention alignment have strengthened. For GP surgeries, compliance is a core component of patient safety, regulatory readiness and operational accountability.
If your practice is reviewing its GP Surgery cleaning arrangements, you can contact our team to discuss a compliant, fully managed solution.
Frequently Asked Questions About NHS Healthcare Cleaning Standards
Yes. Full compliance with the National Standards of Healthcare Cleanliness 2021 became mandatory in November 2022 for NHS healthcare settings. This includes primary care environments operating under NHS frameworks. Healthcare providers are expected to demonstrate adherence through documented cleaning specifications, risk categorisation and structured audit processes.
Functional Risk categories (FR1–FR6) classify each area within a healthcare environment according to infection risk. The assigned category determines cleaning frequency, performance standards and audit requirements. Higher-risk areas require more frequent cleaning and tighter audit controls.
Functional Risk categories must be allocated following a documented risk assessment. This considers factors such as clinical activity, patient contact, exposure risk and room usage. The assigned category should be reviewed if the function of a room changes.
Technical audit frequency is linked to the assigned FR category and local governance requirements. Higher-risk areas are typically audited more frequently than lower-risk administrative areas. Audit results must be documented and retained as evidence of compliance.
A technical audit measures the outcome of cleaning by assessing whether the required standard has been achieved. An efficacy audit evaluates how cleaning is delivered, including adherence to PPE usage, colour coding systems, COSHH compliance and staff training procedures.
The star rating system was introduced under the National Standards to promote transparency. Implementation varies in primary care settings depending on local NHS guidance. However, the underlying requirement for measurable cleanliness performance still applies.
While the Care Quality Commission does not directly enforce the NHS standards, inspectors may review documentation demonstrating infection prevention controls, cleaning audit records, staff training and risk categorisation during inspections.
No. A generic office cleaning schedule is unlikely to meet the structured risk-based framework required under the National Standards of Healthcare Cleanliness. Healthcare environments require documented Functional Risk allocation, defined frequencies and measurable audit processes.
Practices should ensure their contractor understands FR1–FR6 risk categorisation, can evidence structured audits, maintains COSHH compliance, provides trained staff and operates with documented supervision and governance processes.
